The Unmet Need: Who Can Benefit From INSPIRA™ ART Treatment
Forward Looking Statement
This presentation contains express or implied forward-looking statements pursuant to U.S. Federal securities laws. For example, the Company is using forward-looking statements when it discusses its mission, two potential intervention modalities of the INSPIRA ART, the INSPIRA ART’s possible indications and the INSPIRA ART’s potential advantages. These forward-looking statements and their implications are based on the current expectations of the management of the Company only and are subject to a number of factors and uncertainties that could cause actual results to differ materially from those described in the forward-looking statements. Except as otherwise required by law, the Company undertakes no obligation to publicly release any revisions to these forward-looking statements to reflect events or circumstances after the date hereof or to reflect the occurrence of unanticipated events. More detailed information about the risks and uncertainties affecting the Company is contained under the heading “Risk Factors” in the Company’s Registration Statement on Form F-1 filed with the SEC, which is available on the SEC’s website, www.sec.gov.
Our mission is to provide an alternative for invasivemechanical ventilation for acute respiratory patients who continue to deteriorate while being treated by noninvasive ventilation.
▪ Non-invasive ventilation (NIV) – is the delivery of oxygen (ventilation support) via a face mask and therefore eliminating the need of an endotracheal airway.
▪ Invasive mechanical ventilation – is positive pressure delivered to the patient’s lungs via an endotracheal tube or a tracheostomy tube.
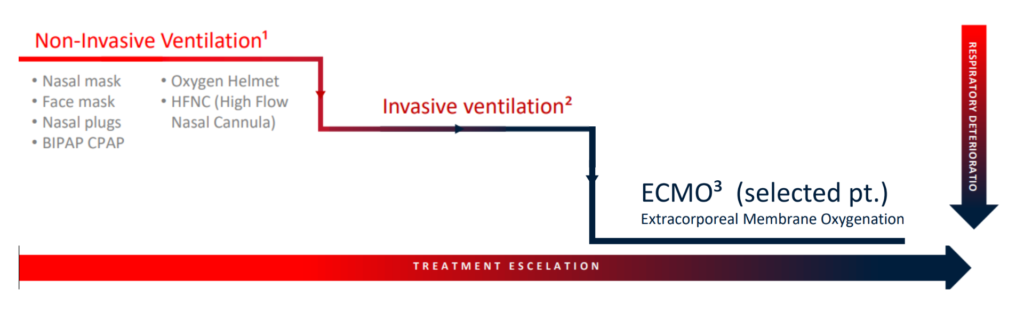
Acute Respiratory Failure: Current Treatment Paradigm
Hypoxemia | Hypercarbia | Hypoxemia & Hypercarbia
1. A Grade 2C recommendation is a very weak recommendation; other alternatives may be equally reasonable.
2. Brown 3rd CA, Walls RM. The decision to intubate. In: The Walls Manual of Emergency Airway Management, 5th ed, Lippincott Williams & Wilkins, Philadelphia 2018. p.3.
3. https://www.elso.org/Portals/0/ELSO%20Guidelines%20General%20All%20ECLS%20Version%201_4.pdf (Accessed on July 23, 2018). Invasive ventilation² Hypoxemia & Hypercarbia
Mechanical Ventilation Has Significant Downsides¹ˉ³
Mechanical ventilation requires intrusive intubation, coma induction, and can be very traumatic for patients:
Potential Risks & Complications:
• Ventilator-induced lung injury (VILI)
• Ventilator-associated pneumonia (VAP)
• Ventilator-induced diaphragmatic dysfunction (VIDD)
• Pneumothorax & tracheomalacia
• Oxygen toxicity of the lung
• Delirium
• Muscular atrophy
High Cost of Treatment:
• Long hospital stays
• Increased complication rate
• Patient re-admissions
• Requires weaning process
• Extended rehabilitation period
1. Am J Respir Crit Care Med Vol. 196, P3-4, 2017. ATS Patient Education Series © 2017 American Thoracic Society
2. Diling Wu et al. Frontiers in pharmacology MINI REVIEW published: 09 May 2019. doi: 10.3389/fphar.2019.00482
3. Kalil AC, Metersky ML, Klompas M, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63:e61-e111.
Why Is It Important to Prevent Invasive Ventilation?
-
Ventilator-induced lung injury (VILI)
Lung injury can be an adverse consequence of mechanical ventilation. This injury is called ventilator-induced lung injury (VILI) and can result in pulmonary edema, barotrauma, and worsening hypoxemia that can prolong mechanical ventilation, lead to multi-system organ dysfunction, and increase mortality¹.
1- UpToDate July 2021
-
Ventilator-induced diaphragmatic dysfunction (VIDD)
Mechanical ventilation itself causes diaphragmatic muscle atrophy; a phenomenon called ventilator induced diaphragmatic dysfunction (VIDD)¹. Controlled mechanical ventilation may lead to a very rapid type of disuse atrophy involving the diaphragmatic muscle fibers, which can develop within the first day of mechanical ventilation
1- UpToDate July 2021
-
Ventilator-associated pneumonia
Ventilator-associated pneumonia (VAP)¹ is a type of hospital-acquired pneumonia (HAP) that develops after more than 48 hours of mechanical ventilation. VAP is a common and serious problem in the intensive care unit that is associated with an increased risk of death
1- UpToDate July 2021
-
Ventilator-associated pneumonia
Ventilator-associated pneumonia (VAP)¹ is a type of hospital-acquired pneumonia (HAP) that develops after more than 48 hours of mechanical ventilation. VAP is a common and serious problem in the intensive care unit that is associated with an increased risk of death.
1- UpToDate July 2021
-
Negative consequences of sedation resulting from mechanical ventilation
Administration of analgesia and sedation to ensure patient comfort and facilitate mechanical ventilation must be balanced against the known negative consequences of excessive sedation Deep sedation, especially early during mechanical ventilation, is associated with prolonged time toliberation from mechanical ventilation, longer ICU stays, longer hospital stays, and increased mortality¹.
1-Pearson, Steven D., and Bhakti K. Patel. “Evolving targets for sedation during mechanical ventilation.” Current opinion in critical care 26.1 (2020): 47
-
Reduce ventilator-induced lung injury
The severity of VILI depends both on the degree (as determined by ventilator settings) and duration of the mechanical insult applied to the lungs¹.
-
Reduce ventilator-induced diaphragmatic dysfunction
Increased duration of mechanical ventilation is associated with decreased diaphragmatic force².
-
Reduce ventilator associated pneumonia
VAP is reported to affect 5–40% of patients receiving invasive mechanical ventilation for more than 2 days, with large variations depending upon the country, ICU type, and criteria used to identify VAP³.
1-Marini, John J., and Patricia RM Rocco. “Which component of mechanical power is most important in causing VILI?.” (2020): 1-3.
2-Hermans, Greet, et al. “Increased duration of mechanical ventilation is associated with decreased diaphragmatic force.” Critical Care 14.1 (2010): 1-1.
3-Papazian, Laurent, Michael Klompas, and Charles-Edouard Luyt. “Ventilator-associated pneumonia in adults: a narrative review.” Intensive care medicine 46.5 (2020): 888-906.
Who Can Benefit From The INSPIRA™ ART System?
INSPIRA™ ART System Offers Two Intervention Modalities
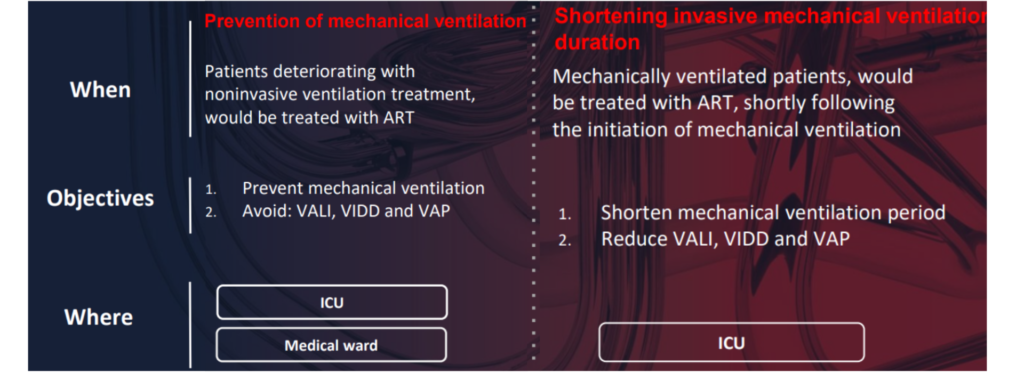
Possible Indications
INSPIRA™ ART may be used for the treatment of acute respiratory failure patients leading tohypoxemia, hypercarbia or both who continue to deteriorate while being treated with noninvasive ventilation.

All indications are subject to testing in human clinical trials
Potential Advantages – The Patient’s Perspective
INSPIRA™ ART may be applied during non-invasive ventilation stage to prevent mechanical ventilation: patient is awake, mobile and breathes spontaneously
- Immediate oxygen saturation elevation and stabilization
- Decreased breathing efforts
- Patient can eat and drink
- Patient can communicate their symptoms and needs to the medical staff
- Patient can communicate with family and friends
- No need for sedation – delirium can be prevented
- Muscle mass loss can be prevented
- Avoiding all forms of complications associated with MV
- Reduction of mortality rate
The Company’s product has not yet been tested or used in humans and has not been approved by the U.S. Food and Drug Administration (FDA) or the CE or other required regulatory agencies.
INSPIRA™ ART treatment* may be added to mechanically ventilated patients
- Reduction of ventilation period
- Less aggressive ventilation –less PEEP, less driving pressures >>> reduced barotrauma and volutrauma
- Reduction of forms of complications associated with MV
- Reduction of mortality rate
* INSPIRA ART Treatment – Early extracorporeal blood oxygenation with 1-1.5 liters of blood.
The Company’s product has not yet been tested or used in humans and has not been approved by the U.S. Food and Drug Administration (FDA) or the CE or other required regulatory agencies.
Potential Advantages – The Hospital Perspective
- Minimize the need for a medical team with prior experience with extracorporeal respiratory systems
- Reduced length of stay >>Increased patient throughput
- Reduced staffing
- Smaller Cannula (compared to ECMO’s cannulas) may prevent the need for surgical access team
- Reduced costs associated with mechanical ventilation complications
- Reduction of patient load in ICU
Potential Advantages – The Medical Team Perspective
- would be able to offer an alternative to mechanical ventilation
- Self priming system results in less human errors
- No prior extracorporeal respiratory systems experience is needed
- Cannula size will allow ICU physicians to insert it without a surgeon involvement


